A11) Dysphagia and chest pain
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with dysphagia.
- Review the DDx considerations in a patient with dysphagia.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with dysphagia.
History
Physical Exam
Labs
Provisional Diagnosis
Potential Acuity
What is your assessment of the likely acuity for this patient?
First Imaging Study
What is the first imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
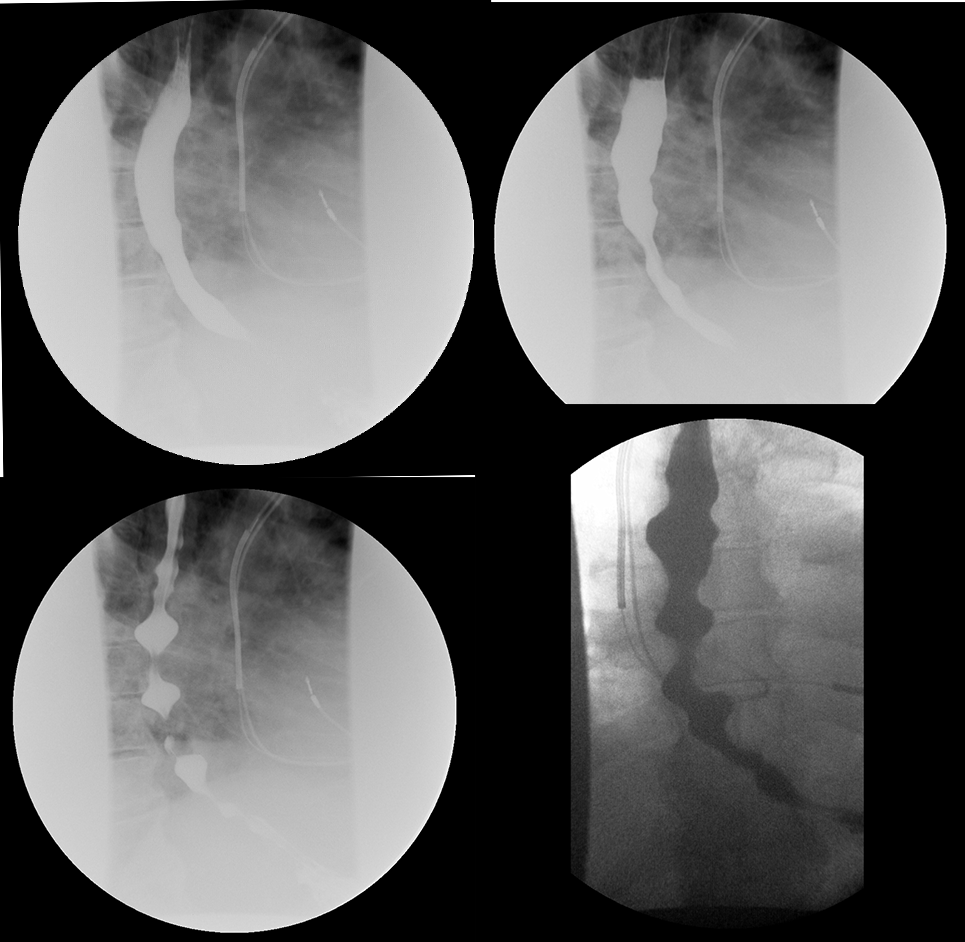
Barium swallow study
What best describes the findings on the barium swallow study?

Watch our video
Second Imaging Study
What is the next imaging study you will order?
What is your Diagnosis now that you have seen the imaging results?
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Assessment and Plan
Please provide your assessment and plan for this patient
Lessons Learned:
- A barium swallow may be performed in patients with dysphagia to assess the structure and function of the pharynx and esophagus.
- A corkscrew or rosary bead appearance of the esophagus on barium swallow is indicative diagnosis of DES.
- Follow up testing with manometry should be conducted in DES patients to confirm the diagnosis and rule out achalasia. This is an important part of the workup as the barium swallow is not highly sensitive or specific for diffuse esophageal spasm. For example, less than 5% of patients with diffuse esophageal spasm have a “corkscrew esophagus” on the barium swallow study. The barium swallow study more often presents with non-peristaltic contractions.
- Calcium channel blockers and nitrates may alleviate symptoms. If the patient has symptoms refractory to medical treatment, Botox injections may be indicated to cause temporary paralysis of the esophageal body. The last option would be an esophageal myotomy. However, this is considered when other treatments don’t work due to lack of long-term studies evaluating patient outcomes.
- Diffuse esophageal spasm may present similarly to angina considering that it is relieved by nitrates.
Socioeconomic Factors:
- Diffuse esophageal spasm is more likely to occur in obese patients since it has an association with hyperlipidemia, hyperglycemia, and hypertension. Patients with low-income who live in areas with poor access to nutritional foods may be more likely to have this diagnosis.
- Older age and psychiatric conditions like anxiety/depression are other common risk factors in the development of diffuse esophageal spasm.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.

{kind=link}